"How Do Fusions Compare" Dr Glenn Butterman
- Paradigm Biodevices Inc.
- Our Blog
- Hits: 4636
This paper is only available as a PDF. To read, Please Download here.
BACKGROUND CONTEXT
Achieving spinal fusion requires bone graft and is most reliable using an anterior/posterior technique. Anterior fusion, due to the large bony surface area between the vertebral bodies, results in reliable fusion. Instrumentation which provides stability, also increases the fusion rate. The bone graft for the posterior fusion may come from a variety of sources. Historically, bone graft was obtained from the iliac portion of the patient's own pelvis, IBG, but this may result in additional postoperative pain. Alternatives are currently the most common form of bone graft, but there is very little knowledge as to the superiority of one alternative over another.
PURPOSE
To determine the ability to achieve a solid posterior spinal fusion using sources of bone graft derived from IBG, bone morphogenic protein (BMP), or from donor bone combined with stem cells derived from either autologous bone marrow aspirate (BMA) or donor bone, fat, or amniotic membrane/fluid.
STUDY DESIGN/SETTING
Prospective randomized single-blinded clinical study of 6 comparative groups with 27 patients in each group.
PATIENT SAMPLE
Adults with advanced degenerative disc disease (DDD) who underwent single-level lumbar spinal fusion.
OUTCOME MEASURES
Outcomes included self-assessment of back and leg pain, pain drawing, ODI, pain medication usage, and procedure success. High resolution CT scans at one year postoperative assessed fusion rates between groups. Costs of graft materials were compared.
METHODS
Outcomes were obtained prospectively. Patients were enrolled over a 7-year period and followed for 2-4 years. All single-level circumferential fusions used BMP anteriorly, instrumentation, and patients were randomized into 6 groups with a different type of bone-graft used posteriorly.
RESULTS
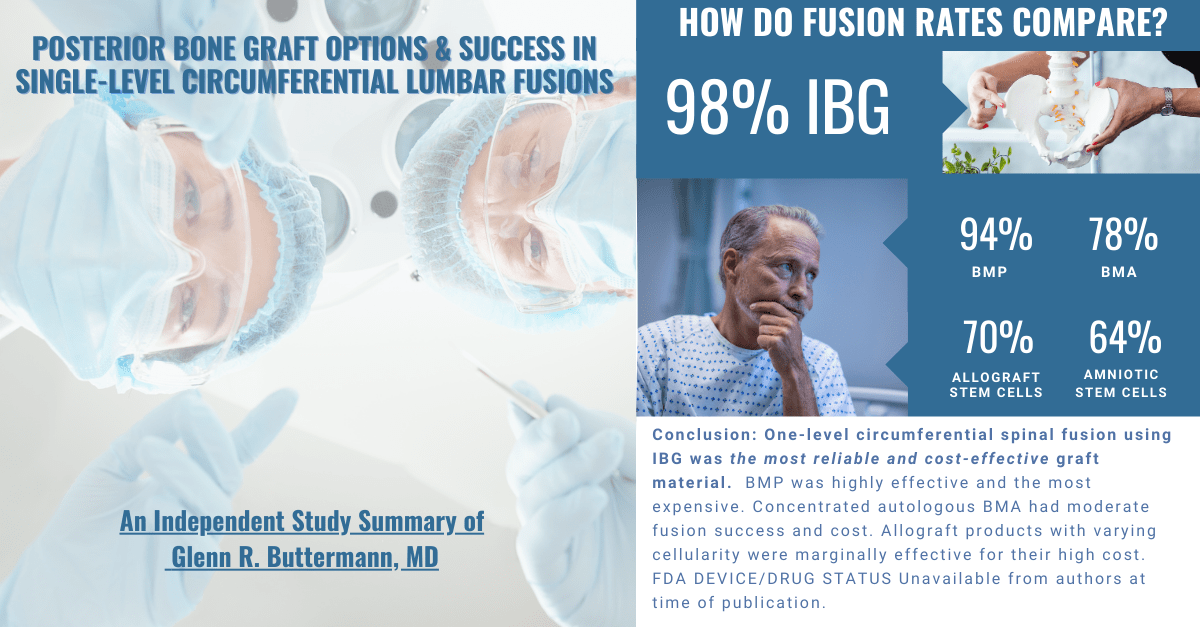
CT scans found solid interbody fusion in 98% of patients. However, solid posterior fusions varied between groups: 98% IBG, 94% BMP, 78% concentrated BMA, 70% bone allograft stem cells, and 64% each for amniotic tissue and fat derived stem cells. Clinical improvement was significant from preop to 2-4 year follow-up within all groups (p < .01 for all outcomes scales). Outcomes were similar between all groups for all outcomes measures. Outcomes were independent of posterior fusion status, however, adjacent level degenerative conditions showed a trend to adversely affect outcomes.
CONCLUSIONS
One-level circumferential spinal fusion using IBG was the most reliable and cost-effective graft material. BMP was highly effective and the most expensive. Concentrated autologous BMA had moderate fusion success and cost. Allograft products with varying cellularity were marginally effective for their high cost.
FDA DEVICE/DRUG STATUS
Unavailable from authors at time of publication.